

The prenatal to age 3 (PN-3) period is the most rapid and sensitive period of development, and it sets the foundation for long-term health and wellbeing. All children deserve the opportunity to be born healthy and raised in nurturing, stimulating, stable, and secure care environments with limited exposure to adversity. Unfortunately, many children lack the opportunities they deserve, and these disparities are often influenced by state policy choices.
To date, states have lacked clear guidance on how to effectively promote the environments in which children can thrive. This Prenatal-to-3 State Policy Roadmap identifies the evidence-based investments that states can make to foster equitable opportunities for infants and toddlers.
The science of the developing child points to eight PN-3 policy goals that all states should strive to achieve to ensure that infants and toddlers get off to a healthy start and thrive. Five state-level policies and six strategies positively impact at least one of these PN-3 policy goals, based on comprehensive reviews of rigorous research. When combined, the policies and strategies create a system of care that provides broad-based economic and family supports, as well as targeted interventions to address identified needs.
This Roadmap helps each state monitor its progress on all 11 effective solutions and on 20 child and family outcome measures that illustrate the health, resources, and wellbeing of infants, toddlers, and their parents in each state. The Roadmap also measures the progress states are making to reduce racial and ethnic disparities in opportunities and outcomes. The framework below illustrates the alignment between the eight policy goals and the 11 evidence-based policies and strategies that impact each goal.
Based on comprehensive reviews of the most rigorous evidence available, the Prenatal-to-3 Policy Impact Center identified five effective policies and six effective strategies that foster the nurturing environments infants and toddlers need. For each of the five policies, the evidence points to a specific policy lever that states can implement to impact outcomes. For the six strategies, the evidence clearly links the strategy to PN-3 outcomes, but the current evidence base does not provide clear guidance on how states should implement each strategy to positively impact outcomes.
The 11 effective solutions are not implemented similarly across all states, leaving children and families across the US with a patchwork of benefits and unequal outcomes. In this Roadmap, we analyze the progress that each state has made in adopting and implementing the most effective policies and identify the states leading the way on the effective strategies.
Only four states—California, the District of Columbia, Massachusetts, and New Jersey—have adopted and fully implemented all five effective policies. “Fully implemented” means that families in the state can currently access the level of benefits that rigorous research states is necessary to impact PN-3 outcomes. Eight states have fully implemented four out of the five policies. Yet, even among states that have implemented a given policy, the generosity and reach of the policy varies considerably across states, which is discussed in detail in subsequent sections of the Roadmap. To date, seven states—Georgia, Mississippi, North Carolina, South Carolina, Tennessee, Texas, and Wyoming—have not fully implemented any of the effective policies.
The focus of this year’s Roadmap is on the progress that states have made over the last year to build stronger and more equitable prenatal-to-3 systems of care. The pandemic caused substantial hardship for many families, particularly families of color, and it exposed how essential economic security, health care, paid leave, and stable child care is for all of us. A year ago, states were reeling from massive unemployment and limited economic activity, and many were facing budget shortfalls and considering cuts to services. Although many are still struggling, federal stabilization efforts have helped many families avoid complete catastrophe and have provided states with unprecedented levels of investments in many of the policies and strategies in this Roadmap. Rather than experiencing a period of retrenchment, many states have moved forward!
Since the last Roadmap, an additional five states have fully implemented at least one of the five Roadmap policies—Missouri implemented two policies. Missouri and Oklahoma adopted and fully implemented Medicaid expansion, Massachusetts fully implemented a 12-week paid family leave program, and three states—Florida, Missouri, and New Mexico—fully implemented a state minimum wage of at least $10.
In addition to the progress of these five states, many more states seriously considered legislation to adopt one of the evidence-based policies, passed legislation to enhance the benefits, or will fully implement one of the policies in the next few years. For example:
States also invested in the evidence-based strategies this past year through legislative or administrative action. For example:
The State Policy Roadmap provides extensive information on each of the effective policies and strategies, including the impact that each solution has on the eight PN-3 policy goals, the choices that states can make to effectively implement them, the progress states have made in the past year toward implementation, and how states vary in their generosity and reach of the policies and strategies. Throughout the Roadmap, there are over 100 data points and indicators of policy implementation that offer insight into the variation in state policy choices.
The purpose of states’ implementing effective PN-3 solutions is to improve the wellbeing of infants, toddlers, and their parents, and to reduce long-standing disparities in outcomes by race and ethnicity. Tracking progress on the following key PN-3 outcomes allows each state to determine the health and wellbeing of children and families in the state and to identify which PN-3 policy goals are lagging and should be prioritized.
National data on these outcomes predate the pandemic, therefore it is likely that family wellbeing is worse than what is illustrated in the Roadmap. But, the data provide an important portrait of how child and family wellbeing varies based on the state in which the family lives.
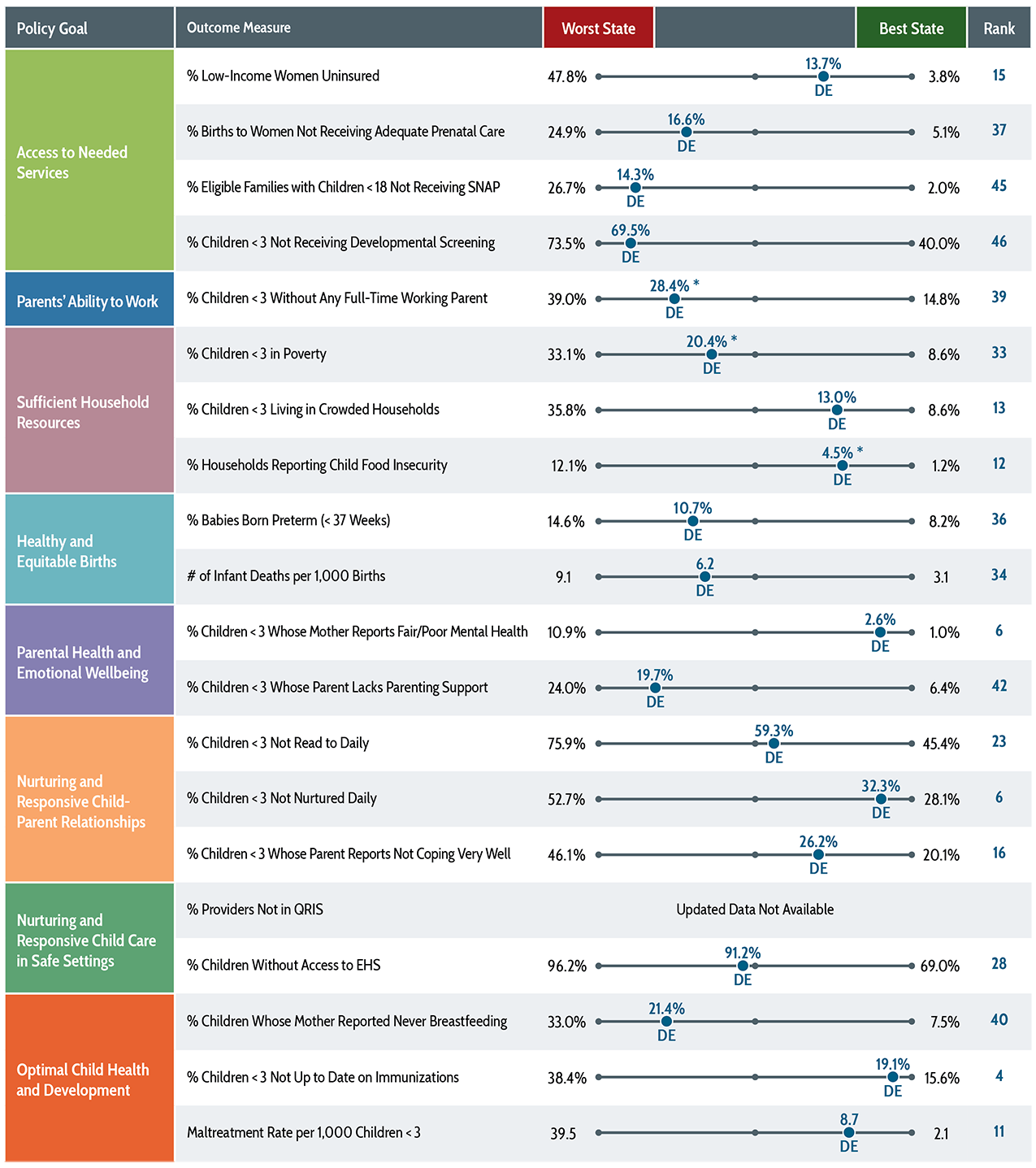
Wide variation exists in the wellbeing of children and families across states. The data below illustrate the range on each outcome between the state in which children and their parents are faring the best, and the state in which they are faring worst, and demonstrates where the state fits within that range.
On some outcomes, such as insecure employment and preterm births, the percentage of children or families who are struggling in the best states is approximately half what it is in the worst states. However, on other outcomes, the differences are much larger. For example, the percentage of low-income women of childbearing age who lack health insurance in Texas (47.8%) is 15 times higher than it is in the District of Columbia (3.8%); and the rate of child maltreatment is 18 times higher in West Virginia than it is in Pennsylvania.
Importantly, the “best” state does not necessarily indicate a target for all other states to strive toward; even in the best states, many children and families are struggling. For example, Minnesota reports the lowest, or best, percentage of children who did NOT receive a developmental screening, but in that state still 40% of children are not screened for potential delays that can identify the need for intervention. Similarly, Minnesota also has the best rate of children receiving all of their required immunizations, but the percentage of infants and toddlers who are not fully immunized is over 15%. The daily reading outcome measure provides another example of an outcome on which all states can improve; Texas families report that over 75% of parents do not read to their infants and toddlers daily, which is the highest, or worst, percentage in the country. Vermont families report the best rate of daily reading, but over 45% of children are not read to daily in the state.
In addition to measuring where states are relative to one another, it is vital that states collect and share information on how families of different race and ethnic groups and socioeconomic statuses fare on these outcomes. For most of these measures, national data are not available that can adequately measure subgroup differences within a state, because of small sample sizes. The outcomes and demographic characteristics sections of the Roadmap provide each state with detailed information on these important measures, and where possible, the data are presented by race and ethnicity.
This Prenatal-to-3 State Policy Roadmap provides each state with information not only on how the state is doing, but how each state can better support the healthy development of infants and toddlers. Each year, the Prenatal-to-3 Policy Impact Center will update this Roadmap to track states’ progress on adopting and implementing the best investments that states can make, based on the most rigorous evidence to date. We will also measure improvements in the overall wellbeing of infants and toddlers, and their parents in each state, and whether states are closing persistent racial and ethnic gaps in wellbeing. Finally, we will continue to monitor and contribute to the growing evidence base to identify additional effective solutions to promote healthy development and family stability.
The science is clear with regard to the conditions necessary to help children thrive. The evidence now exists on how states can invest in effective policies and strategies to foster these conditions. This Roadmap is meant to serve as a guide for states as they undertake these important efforts to ensure all children have the opportunities they deserve.