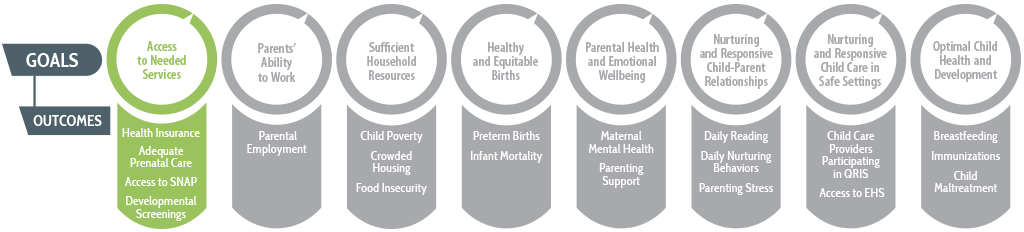
Ensuring access to the resources and services that parents and children need is foundational to building a prenatal-to-3 system of care. States provide a number of benefits and programs to children and families, based on varying eligibility criteria and modes of delivery. However, use of services among families who are eligible varies considerably from state to state: Between two children in different states with identical needs, one may receive a benefit that the other does not, a situation leaving many without the services that help them to thrive. Families of color, in particular, are less likely to receive services even though they are eligible, as demonstrated by research on programs such as Medicaid, WIC, and Early Intervention (EI) services.1,2 For example, in a study about EI services, eligible Black children at age 2 were found to be 5 to 8 times less likely to receive services than White children, depending on the eligibility category.3
States have the ability to increase families’ and children’s access to services through three primary pathways:
- Expanding eligibility criteria;
- Reducing administrative burden and barriers to services; and
- Screening for the specific needs that families and their children have and connecting them with the precise services they need.
Expanded Eligibility Criteria
States have the flexibility to determine who is eligible for many programs and services, including programs largely funded by the federal government. Determinations about who is eligible for a service can be driven by whether a state has adopted a specific policy (for example, paid family leave or expanded income eligibility for health insurance), the broad or narrow criteria the state uses to determine whether someone is eligible (for example, criteria for Early Intervention services or child care subsidies), or whether to include or exclude certain populations that are not automatically eligible (for example, some states use state funds to provide services to immigrant families and children). These decisions drive variation in whether two children or parents with similar needs, but in different states, receive similar help.
Fewer Barriers to Services and Reduced Administrative Burden
Families experience different levels of barriers accessing resources and care. For some families, barriers are low and accessing resources is often simple, but for other families, multiple barriers (e.g., lack of transportation or time, exclusivity, lack of support, high costs, etc.) may make it difficult to access resources and care needed to help their families thrive. States can make choices that ease the barriers individuals and families face in accessing resources and care, and in doing so, may also subsequently improve additional indicators of families’ wellbeing as a result of increased use of needed services and programs. For example, states can support innovative program models, such as group prenatal care models, that seek to improve the accessibility of care (e.g., through an alternative care model and the integration of peer support).
Administrative burden refers to the barriers that increase the costs—time, money, and psychological distress—of applying for and maintaining eligibility in a public assistance programs. Administrative burden policies come in many forms, such as requiring that recertification for benefits take place in person rather than remotely, or that recertification take place every 3 months rather than 12, or that a host of documents be presented to prove eligibility. Moreover, the policies can result from intentional or inadvertent features of regulations that states put in place.4 Regardless of the intentions, administrative burden policies are largely costly and inefficient, and they reduce the use of services among those who are eligible. Because state resources are generally scarce, reasonable policies are needed to ensure that only families who are eligible receive the intended services, but states have found methods to reduce fraud while also reducing unnecessary burdens on eligible families.
Screenings and Connections to Needed Services
Identifying needs early and addressing them immediately helps to reduce the need for later services (and saves money).5 An adequate system for screening and connections requires four components: (1) screening to identify the precise services that are needed, (2) referring and connecting the family to the needed services, (3) serving the family to address the need, and (4) monitoring outcomes to ensure the need is addressed. A breakdown in any of these links to services threatens the health of the system and may compromise improvements in outcomes. Our current systems often focus on screening, yet neglect to document the needs of the families, the services rendered, or the improvements made in family and child wellbeing.
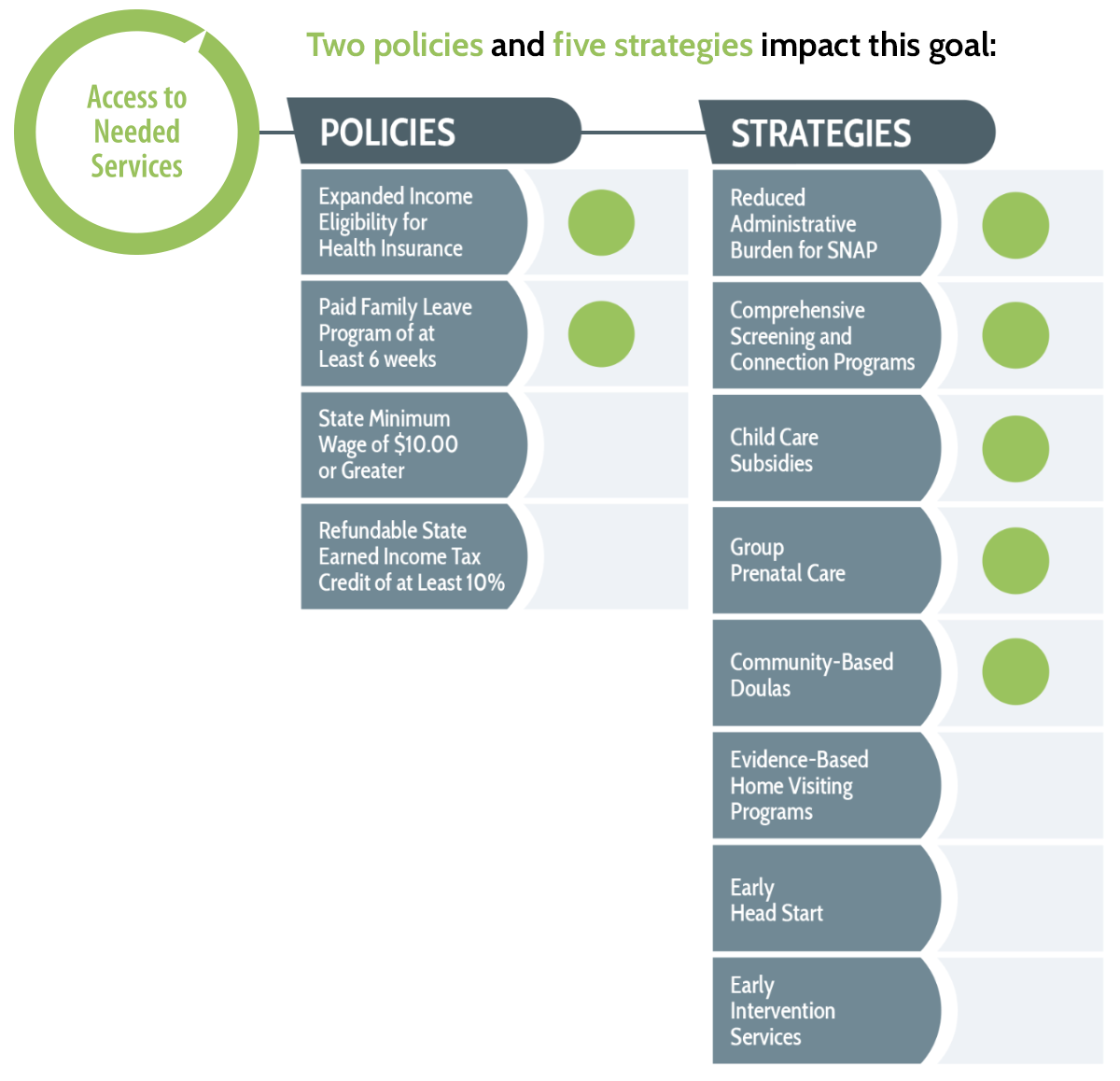
Through our comprehensive reviews of rigorous research, we have identified policies and strategies that provide states with key opportunities to remove obstacles that prevent families from participating in the programs intended to help them thrive. Next is a closer look at these policies and strategies and an overview of important outcome measures that states should use to track their progress toward removing barriers to access.